As recently as 2017, regarding clinical implementation of Acuros,
Yan, et al. admitted that “further investigation and clarification is needed about which dose reporting mode (dose-to-water or dose-to-medium) should be used in clinics.” In reviewing the literature, there appears to be a slight tendency toward using D
m for patient calculations, and
C-M Ma and Jisheng Li agree that D
m is recommended for dose prescription and outcome analysis. With that said,
Chen et al. suggest using D
w when calculating to quality assurance phantoms (unless the phantom is a water phantom) due to the CT-to-biological materials conversion potentially not performing well for non-biological materials such as plastics.
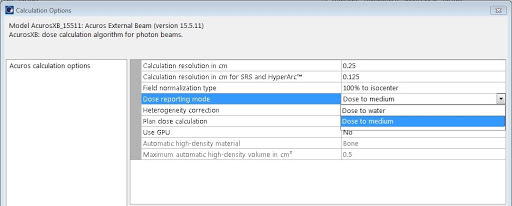
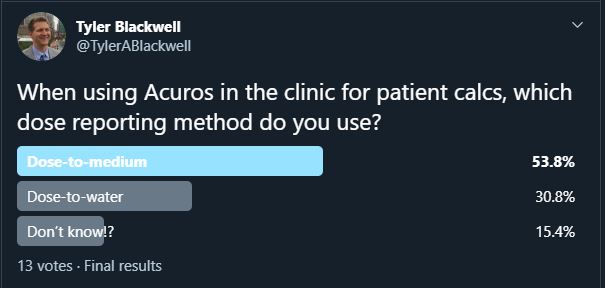
With the debate being far from settled, which reporting method do you use? A Twitter poll of clinical users revealed that 53.8% prefer Dm while 30.8% use Dw in the clinic for patient calculations (and 15.4% aren’t sure). Two other votes were provided via email, both in favor of dose-to-medium reporting. What does your clinic use?

Leave a comment