RadOnc News
Podcasts in Radiation Therapy
Check out Radformation’s favorite podcasts in radiation therapy.
Radformation’s medical physicists break down highlights from the 2018 ASTRO Guidelines for Whole Breast and discuss how EZFluence automation allows for suc
Radformation’s medical physicists break down highlights from the 2018 ASTRO Guidelines for Whole Breast and discuss how EZFluence automation allows for successful planning of these cases.
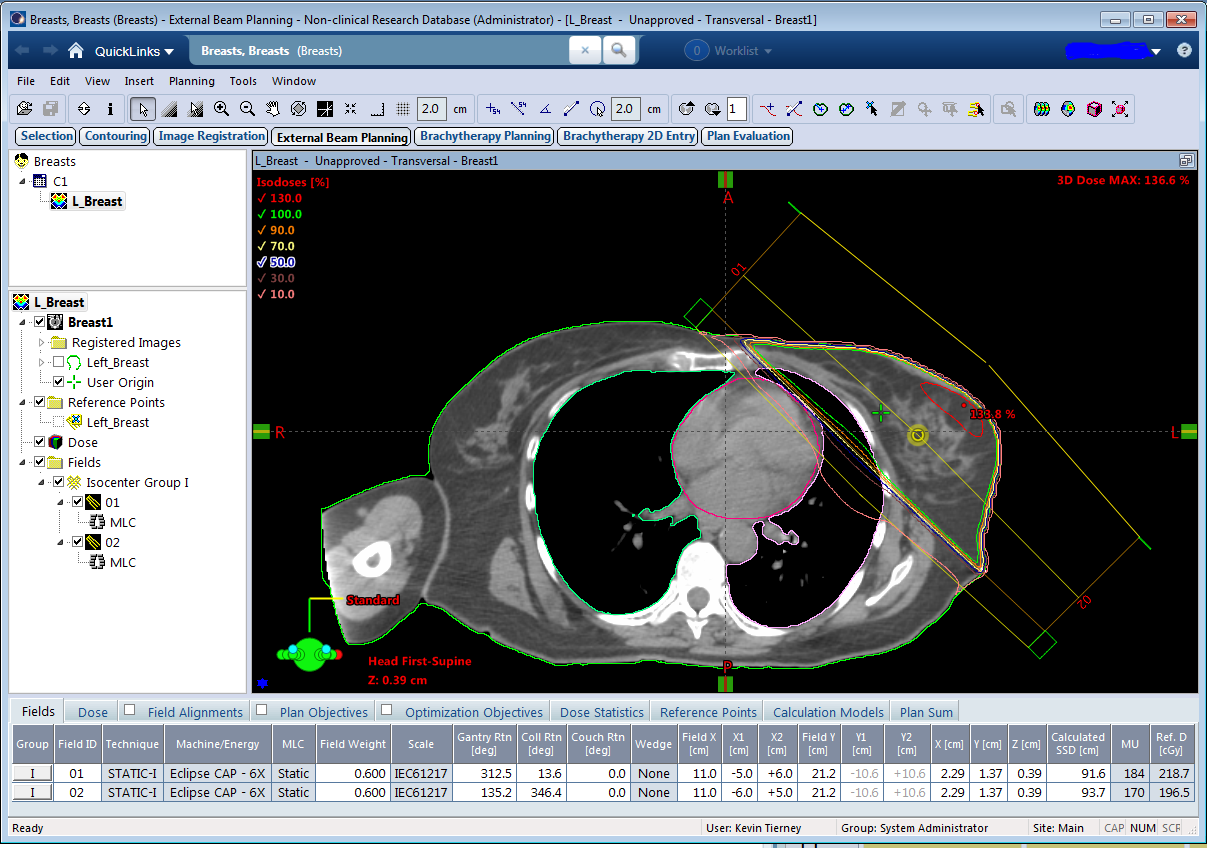
ABOVE: Screenshot of a conventional tangent field setup for a Whole Breast Irradiation (WBI) treatment in the Eclipse Treatment Planning System.
In March of this past year ASTRO issued their latest clinical guidelines for whole breast radiation therapy . We look at some of the key questions raised by the issued guidelines, and discuss ways Radformation’s EZFluence can assist planners in following these guidelines quickly and with increased safety.
Q: Is Hypofractionated WBI (Whole Breast Irradiation) really the best solution for patients with breast cancer? If so, why?
A:While there is no benefit to tumor control or side effects, hypofractionated radiation therapy is faster and more cost efficient than alternatives. This is significant, as Dr. Reshma Jagsi of U of M (Ann Arbor) states that “A shorter course of radiation equates to more time with family, less time away from work and lower treatment costs.” Planning for these hypofractionated cases will not change significantly compared to conventional techniques, but the new ASTRO guidelines recommend more care be taken to maximize dose homogeneity within the breast while sparing normal tissues.
Q: What changes to treatment plan quality are recommended by the ASTRO 2018 guidelines?
A: With respect to Whole Breast Irradiation, new emphasis is placed on target dose homogeneity within the breast. Prior recommendations required homogeneity along the central axis of +/-7%. The new guidelines recommend achieving a coverage goal of 95% of the breast volume receiving 95% of the prescription dose while also reducing the V105% as much as possible. Meeting these goals will require more time and effort during treatment planning with more complex Field-In-Field Segments and mixed energies when necessary.
EZFluence makes implementing these recommendations simple by:
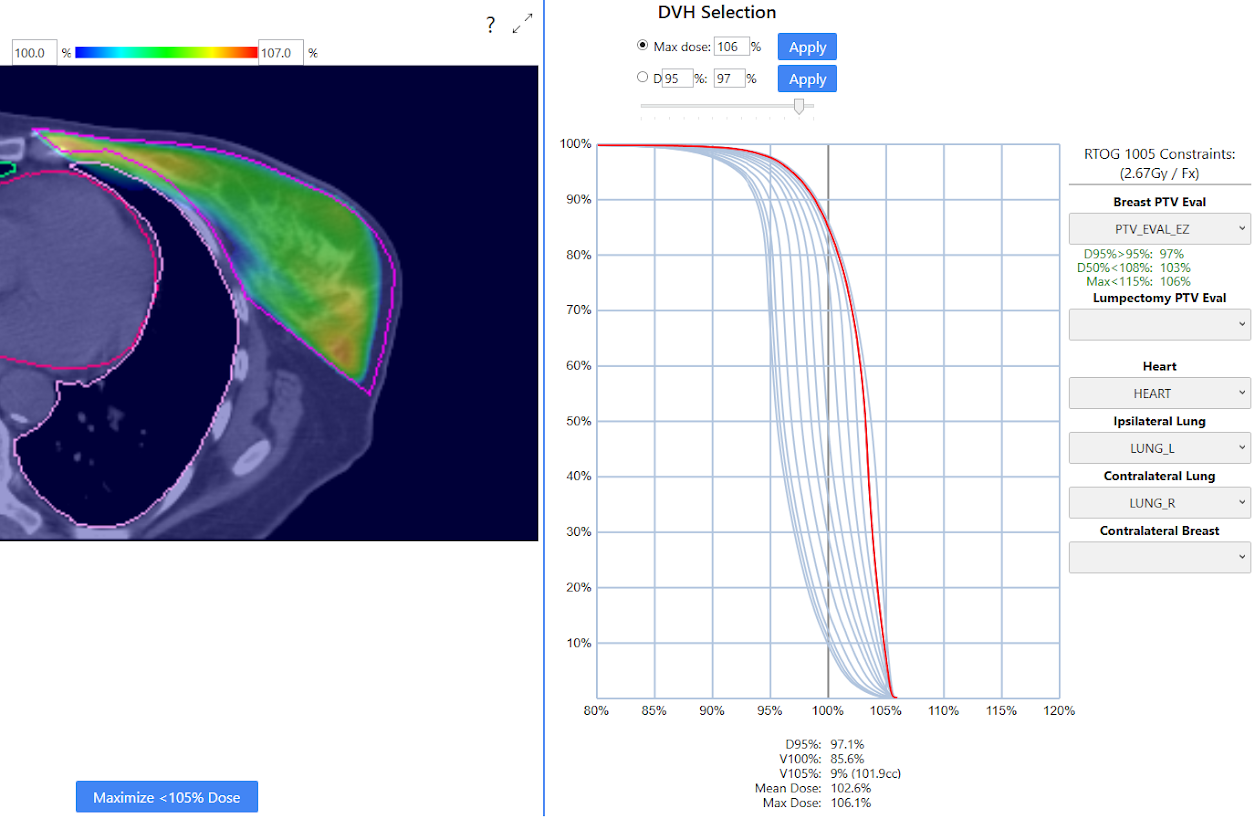
ABOVE: Screenshot of automated plan generation in EZFluence. DVH Window on right allows planners to quickly compare trade-off between breast coverage and V105% on a variety of plans.
Q: What is the preferred technique for treatment planning?
A: To maximize homogeneity and tumor coverage, ASTRO recommends “three-dimensional conformal (3D-CRT) treatment planning with forward planned, field-in-field technique”. EZFluence can produce either Field-in-Field (with a user-specified number of subfields and minimum MU per subfield) or electronic compensator treatment plans.
Though not discussed in these guidelines, IMRT or VMAT may be necessary for Internal Mammary Lymph Node coverage and/or when there is prohibitively high lung or heart dose when treating with wide tangents: “Breast tumors may be appropriate for IMRT, but often require further review regarding coverage for the IMRT technique per payer guidelines. For example, IMRT is often appropriate for left breast cases due to cardiac and pericardial structures, but is not routinely appropriate for the right breast.” [2017 ACRO Billing and Coding Guide, pg. 85]
Q: When is a Radiation boost appropriate?
A: The latest ASTRO guideline summary states:
Q: Sequential Boost or Integrated Boost?
A: The ASTRO guideline gives the following Conditional recommendation: “At this time, evidence is strongest in support of sequential administration of the boost after whole breast treatment; therefore, outside the context of trials, sequential boost is currently recommended.”
While Sequential Boosting is recommended, there have been studies looking at integrating the boost dose (e.g. RTOG 1005: 4800cGy in 15 Fx) into the WBI treatment fractionation (4000cGy in 15 Fx) as a “Dose Painted” region. Traditionally, sequential breast boosts are prescribed to a specific depth (e.g. 4cm) which corresponds to the deepest portion of the tumor bed. This is commonly treated with electron or single photon field techniques. However, with more recent emphasis on homogeneity and limiting OAR dose, more clinicians are using volumetric dose when prescribing to the tumor bed. A trend away from the use of electrons can also be seen as concurrent boosting methods look for more improved coverage with smaller hotspots. Photon boosting also has the benefit of a simplified in-room setup for the patient, as a single isocenter may be used and integration into the field-in-field WBI fields is possible, reducing the number of days in which a patient needs to come in for treatment and their time on the table. Furthermore, potential setup errors common with additional shifting to boost fields can be avoided.
For sequential boosts, EZFluence can be used for both the WBI and mini-tangent boost plans separately to provide a homogeneous dose distribution in each case independently. EZFluence version 1.5 (planned release in January 2019) will also support integrated boosts – the user can simply choose the target structure and coverage goal, and for electronic compensator, the optimizer will scale the dose to the target up to achieve optimal coverage without additional field construction. If Field-in-Field is used, additional subfields will be automatically incorporated into your plan to achieve the desired coverage to the boosted region.
Disclaimer
This blog provides general information and discussion about medicine, health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately-licensed physician or other health care worker.
Never disregard professional medical advice or delay in seeking it because of something you have read on this blog or in any linked materials. If you think you may have a medical emergency, call your doctor or 911 immediately.
The views expressed on this blog and website have no relation to those of any academic, hospital, practice or other institution with which the authors are affiliated.

Leave a comment